
Dejan Galič, MD, FEBU, FECSM
urology specialist
He deals with general urology, especially urological oncology and prostate problems, as well as sexual medicine.


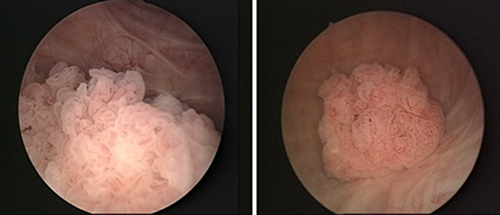
When a tumor is confirmed by cystoscopy, surgical treatment is required. The tumor is excised with an electrical loop through the urethra, and the tumor pieces are sent to a pathologist, who stains the tissue with special dyes and examines it under a microscope. This is how we arrive at a definitive diagnosis, and surgery itself can be the definitive form of treatment. If it turns out that the disease cannot be controlled in this way, the disease involves the muscle layer or recurs, more aggressive therapy is required. The pathologist distinguishes between high-grade and low-grade tumors and how deep the tumor grows into the bladder wall. Depending on the pathologist's report and the patient's general condition (comorbidities, psychophysical condition), we decide on further therapy. Most often, the above-mentioned surgical procedure represents the definitive therapy. The procedure is called transurethral resection of a bladder tumor. As a rule, superficial tumors that do not extend to the bladder musculature and do not recur after additional immuno/cytostatic therapy (BCG, Mitomycin) are treated in this way.
If the tumor extends deeper, to the musculature, through it, or tumors recur despite additional therapy, the bladder must be removed, usually completely (cystectomy). Urine drainage must be ensured, which is achieved by creating a urine reservoir from the intestine and draining it naturally, or through a dry/wet urostomy. The operation can be performed open/classically, through a larger incision in the abdominal wall, or laparoscopically/robotically assisted. The results are comparable, but with the latter two methods, postoperative recovery is faster, blood loss is less, hospitalization time is shorter, and the cosmetic appearance is better.
In case the patient is not fit for surgical therapy due to poor psychophysical condition or serious concomitant diseases, we decide to use radiation therapy in combination with chemotherapy. Radiation therapy is administered in fractions - every day for 5-8 weeks.
Approximately 15% of patients have affected lymph nodes or distant metastases at the time of diagnosis. Chemotherapy is effective in at least 2/3 of cases and is also used before surgery (neoadjuvant chemotherapy) or postoperatively (adjuvant chemotherapy). We decide on a combination of different cytostatics.
Author: asst. Simon Hawlina, MD, FEBU, urologist specialist
Avoiding smoking (Figure 3) is the best prevention. We recommend a healthy lifestyle, avoiding stress, and adequate hydration. If you already have the disease, we recommend regular check-ups with a urologist.

Figure 3: Avoid smoking





Monday - Thursday
Friday
Saturday - Sunday
08:00 - 19:00
08:00 - 16:00
Closed
Copyright © 2025 MD medicina | All Rights Reserved | Quality and safety | Privacy Policy